
TL;DR:
- Accessibility in therapy involves removing physical, digital, and cultural barriers to ensure equitable participation for all clients. Legal mandates like the ADA and Section 504 require healthcare providers to meet standards such as WCAG 2.1 AA and provide inclusive, flexible services. Addressing both structural and emotional accessibility is essential for meaningful engagement, especially among marginalized populations.
Accessibility in therapy is defined as the removal of barriers that prevent individuals from equally participating in mental health services, regardless of disability, background, or circumstance. The term used across professional and legal frameworks is "therapeutic accessibility," and it covers physical spaces, digital platforms, communication methods, and cultural competence. Legal instruments including the Americans with Disabilities Act (ADA) and Section 504 of the Rehabilitation Act set binding standards for providers. Platforms like those operated by Mysafetherapy demonstrate that meeting WCAG 2.1 accessibility guidelines and offering multiple session formats are not optional extras. They are the baseline for equitable care.
Why accessibility in therapy is a legal and ethical obligation
Therapeutic accessibility is not a matter of goodwill. The ADA requires healthcare providers, including telehealth services, to ensure nondiscrimination and provide effective communication aids such as qualified interpreters and real-time captioning, without passing the cost to patients. This applies to every touchpoint: the booking system, the session platform, and any pre-visit materials.
Section 504 of the Rehabilitation Act extends these protections to any organisation receiving federal financial assistance. It mandates that digital properties meet WCAG 2.1 Level AA standards, covering websites, patient portals, telehealth platforms, kiosks, and mobile apps. Large organisations face a compliance deadline in May 2026, making this an urgent operational matter, not a future consideration.
Providers must also make reasonable modifications to their policies and procedures. These include:
- Allowing a support person or carer to join sessions to assist communication
- Offering extended appointment times for clients who need additional processing time
- Providing documents in accessible formats such as large print, audio, or plain language
- Permitting remote interpreters to join telehealth calls without requiring patients to arrange their own
Pro Tip: Many providers focus on session-level accessibility and overlook the digital front door. An inaccessible booking page or patient portal can block access entirely before a single session takes place. Audit your scheduling system and pre-visit communications first.
| Legal framework | Key requirement | Scope |
|---|---|---|
| ADA Title II and III | Communication aids, nondiscrimination | All healthcare providers, including telehealth |
| Section 504 | WCAG 2.1 AA digital compliance | Organisations receiving federal funds |
| WCAG 2.1 AA | Screen reader compatibility, captioning, keyboard navigation | Websites, apps, portals, telehealth platforms |
What practical barriers limit therapy access for disabled and marginalised communities?
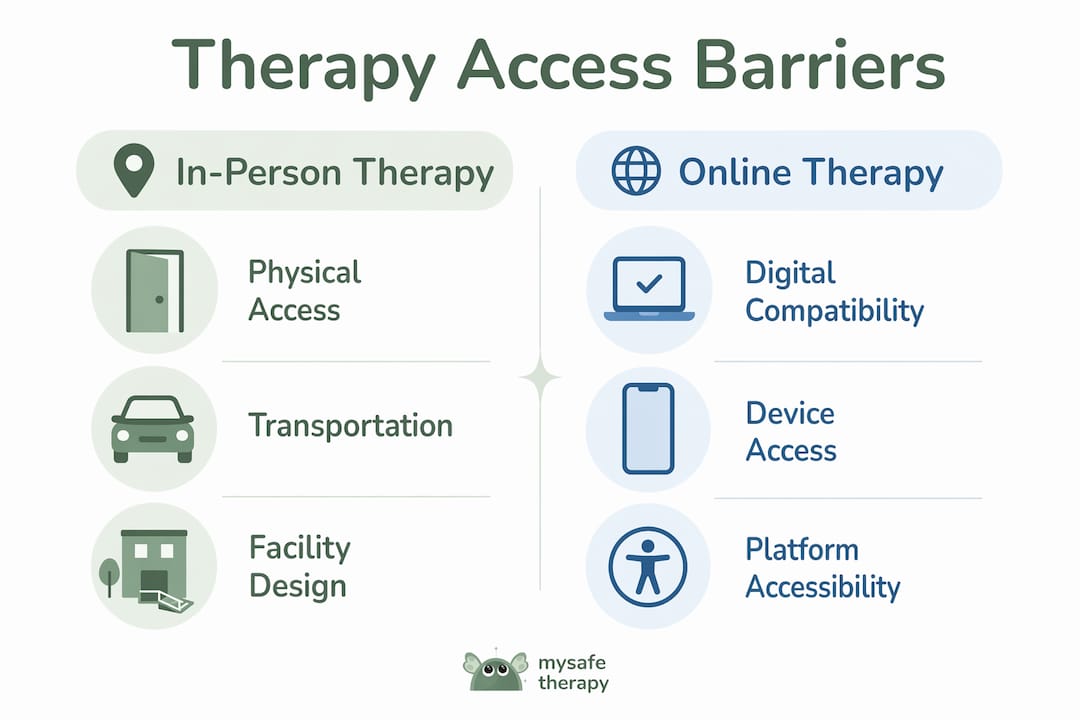
Barriers to therapy access extend well beyond legal compliance. Online therapy can both remove and create barriers for disabled people, depending on how platforms are designed and what assumptions providers make about users' circumstances.
Physical barriers remain significant for many. Inaccessible premises, unreliable public transport, and the energy demands of travelling to appointments exclude people with mobility impairments, chronic fatigue conditions, and sensory disabilities. These are not edge cases. They represent a substantial portion of the population seeking mental health support.
Digital barriers present a different set of problems. Platforms that lack captioning, screen reader compatibility, or keyboard navigation exclude Deaf users and those with visual impairments. Assumptions about private devices and reliable broadband ignore the realities of many disabled people's lives. Limited broadband, device access, and low digital literacy disproportionately affect rural, low-income, and disabled populations, meaning telehealth can widen inequity rather than close it.
Financial and structural barriers compound these issues. The shortage of therapists trained in disability-aware practice, rigid appointment systems, and high session costs all reduce access. Clients who need longer sessions or more frequent contact face higher costs with no corresponding support.
| Barrier type | In-person therapy | Online therapy |
|---|---|---|
| Physical access | Inaccessible buildings, transport costs | Eliminated for mobility issues, but device access required |
| Communication | Interpreter availability at venue | Remote interpreter integration possible but often absent |
| Financial | Travel costs, session fees | Session fees remain; data costs added |
| Privacy | Separate space guaranteed | Home privacy not guaranteed for all |
| Digital literacy | Not required | Required; excludes some users |
Pro Tip: Offering clients a genuine choice of therapy format, including video, phone, chat, and asynchronous options, is one of the most direct ways to reduce access barriers. A single-format service excludes by design. Read more about choosing the right format for different accessibility needs.
How does technology affect accessibility in therapy?
Technology is the most significant variable in therapy accessibility today. When designed correctly, telehealth eliminates transport barriers, reduces stigma through private access, and extends reach to rural and mobility-impaired clients. When designed poorly, it creates a new layer of exclusion.
The benefits of accessible telehealth are well documented. Clients who previously could not attend in-person sessions due to physical disability, chronic illness, or geographic isolation can now access qualified therapists from home. Evening and flexible session options further expand access for those with caring responsibilities or variable energy levels.
The risks are equally real. Telehealth platforms that fail to integrate captioning, sign language interpretation support, or screen reader compatibility exclude the very populations they could most benefit. Providers cannot require patients to provide their own interpreters or captioners. The ADA guidance is explicit on this point: communication aids are the provider's responsibility.
The digital divide remains the most persistent structural problem. Broadband availability, device ownership, and digital literacy gaps mean that expanding therapy online does not automatically expand access. Telehealth and task-shifting work only if digital infrastructure and policy frameworks actively support equity. Without that, disparities worsen.
Hybrid care models, combining digital sessions with community-based or in-person elements, offer the most equitable approach. They accommodate clients who cannot use digital platforms reliably while retaining the flexibility benefits for those who can.
Pro Tip: When selecting a telehealth platform, check for WCAG 2.1 AA compliance, built-in captioning, keyboard navigation, and the ability to add a remote interpreter. These features should be standard, not add-ons. A platform that fails these checks fails a significant proportion of clients before the session begins.
Why is cultural and emotional accessibility essential in therapy?
Cultural and emotional accessibility is defined as the capacity of a therapy service to make clients from marginalised backgrounds feel genuinely safe, understood, and respected, not merely tolerated. This dimension of access is frequently absent from compliance frameworks, yet it determines whether clients engage at all.
For Black clients and other marginalised groups, access is more than availability. Cultural safety and emotional accessibility shape engagement as much as logistical factors. Clients who anticipate being misunderstood, stereotyped, or required to educate their therapist about their lived experience face an emotional labour cost before the first session begins. That cost is itself a barrier.
The challenges are specific and well-evidenced:
- Black clients frequently report difficulty finding therapists who can engage with their lived realities without distortion or projection
- LGBTQ+ clients face the risk of encountering providers who are not affirming, which can cause harm rather than support
- Clients from refugee or asylum-seeking backgrounds may carry mistrust of institutions that affects their willingness to disclose
- Neurodivergent clients often find that standard therapeutic frameworks do not accommodate their communication styles
Increasing the number of therapists does not resolve these issues on its own. A larger pool of providers who share the same cultural blind spots does not improve meaningful access. Representation among therapists, training in cultural safety, and genuinely affirming practice are the variables that matter. Providers and organisations need to recruit diversely, train consistently, and create feedback mechanisms that surface client experience rather than assume satisfaction.
What strategies can improve accessibility in therapy?
Improving therapy access requires action across multiple dimensions simultaneously. No single intervention resolves the full picture. The following steps reflect the evidence base and the practical realities of service delivery.
- Offer multiple session formats. Video, phone, chat, and asynchronous options accommodate different disabilities, communication preferences, and life circumstances. A step-by-step guide to accessible online therapy can help providers implement these formats correctly.
- Audit the digital front door. Websites, booking systems, and patient portals must meet WCAG 2.1 AA standards. Inaccessible scheduling and pre-visit materials are among the most common access failures and the most preventable.
- Build communication support into every service. Captioning, remote interpreter integration, and plain language documentation should be standard features, not special requests.
- Adopt flexible scheduling policies. Allow clients to reschedule without penalty when disability-related factors intervene. Offer extended session times where needed.
- Recruit and train for cultural competence. Diverse therapist teams and consistent training in cultural safety are prerequisites for emotional accessibility.
- Embed mental health in primary care. Integrating care and using task-shifting to non-specialist community workers expands reach in underserved areas where specialist therapists are scarce.
- Co-design with clients. Solicit feedback from disabled and marginalised clients directly. Accessibility measures designed without input from those affected routinely miss the most significant barriers.
Pro Tip: Conduct an accessibility audit at least annually, covering your website, booking system, session platform, and therapist training records. Pair this with a short client experience survey that specifically asks about access barriers. The gap between what providers assume works and what clients actually experience is consistently larger than expected.
Key takeaways
Accessibility in therapy requires simultaneous action on legal compliance, digital design, cultural safety, and operational flexibility to achieve genuinely equitable mental health access.
| Point | Details |
|---|---|
| Legal compliance is the baseline | ADA and Section 504 mandate communication aids, WCAG 2.1 AA digital standards, and nondiscrimination across all touchpoints. |
| Digital barriers are structural | Limited broadband, inaccessible platforms, and poor digital literacy exclude many disabled and low-income clients from telehealth. |
| Cultural access shapes engagement | For marginalised groups, emotional safety and cultural competence determine whether clients engage, not just whether services exist. |
| The digital front door matters | Inaccessible booking systems and portals block access before a session begins; holistic digital audits are necessary. |
| Multiple formats reduce exclusion | Offering video, phone, chat, and asynchronous therapy removes barriers that a single-format service cannot address. |
Accessibility is more complex than most providers realise
At Mysafetherapy, we see a consistent pattern: providers who believe they have addressed accessibility because they offer online sessions. They have ticked one box. The reality is that accessibility in therapy operates across at least four distinct dimensions, and progress on one does not compensate for failure on another.
The most overlooked dimension is emotional and cultural accessibility. We have observed that clients from marginalised communities often disengage not because a service is technically unavailable, but because the experience of seeking it carries too high an emotional cost. The anticipatory labour of wondering whether a therapist will understand your background, your identity, or your specific disability is a real access barrier. It does not appear in compliance audits.
We also think the sector underestimates how much the digital front door matters. A therapist who is fully trained in disability-aware practice and cultural safety is inaccessible if the booking system requires a level of digital literacy or device capability that many clients do not have. The chain of access is only as strong as its weakest link.
The path forward is not complicated, but it does require providers to stop treating accessibility as a compliance exercise and start treating it as a client experience question. That shift in framing changes everything about how services are designed, audited, and improved.
— MySafeTherapy
How Mysafetherapy supports accessible therapy for diverse needs
Mysafetherapy connects clients across the UK with BACP, UKCP, and NCPS-registered therapists who specialise in a range of needs, including disability-aware practice and culturally affirming care. The platform offers video, chat, and avatar-based sessions, with evening and weekend availability to accommodate varied schedules and energy levels.
Booking is straightforward and designed with accessibility in mind, including clear pricing, flexible session frequency, and the option to switch therapists without friction. Whether you are managing anxiety, trauma, burnout, or a condition that affects how you communicate, Mysafetherapy offers formats that work for your circumstances. Start therapy today and find a therapist matched to your specific needs, on your terms.
FAQ
What does accessibility in therapy actually mean?
Accessibility in therapy means removing physical, digital, financial, and cultural barriers so that all individuals can equally participate in mental health services. It includes communication aids, flexible formats, inclusive platform design, and culturally competent practice.
Are therapy providers legally required to be accessible?
Yes. The ADA and Section 504 require healthcare providers, including telehealth services, to provide communication aids and meet digital accessibility standards without charging patients. Large organisations must comply with WCAG 2.1 AA digital standards by May 2026.
Why is online therapy not automatically more accessible?
Online therapy can create new barriers through inaccessible platform design, assumptions about device ownership and reliable broadband, and the absence of captioning or interpreter support. The digital divide means telehealth can worsen inequity if infrastructure and design do not actively support all users.
How does cultural accessibility differ from physical accessibility?
Cultural accessibility refers to the emotional safety and affirmation clients experience in therapy, particularly those from marginalised backgrounds. It includes therapist representation, training in cultural competence, and the absence of anticipatory mistrust. Physical accessibility addresses built environment and transport barriers.
What is the most common accessibility failure in therapy services?
The most common failure is an inaccessible digital front door. Booking systems, patient portals, and pre-visit materials that do not meet WCAG 2.1 AA standards block access before a session begins, even when the therapy itself is fully accessible.