TL;DR:
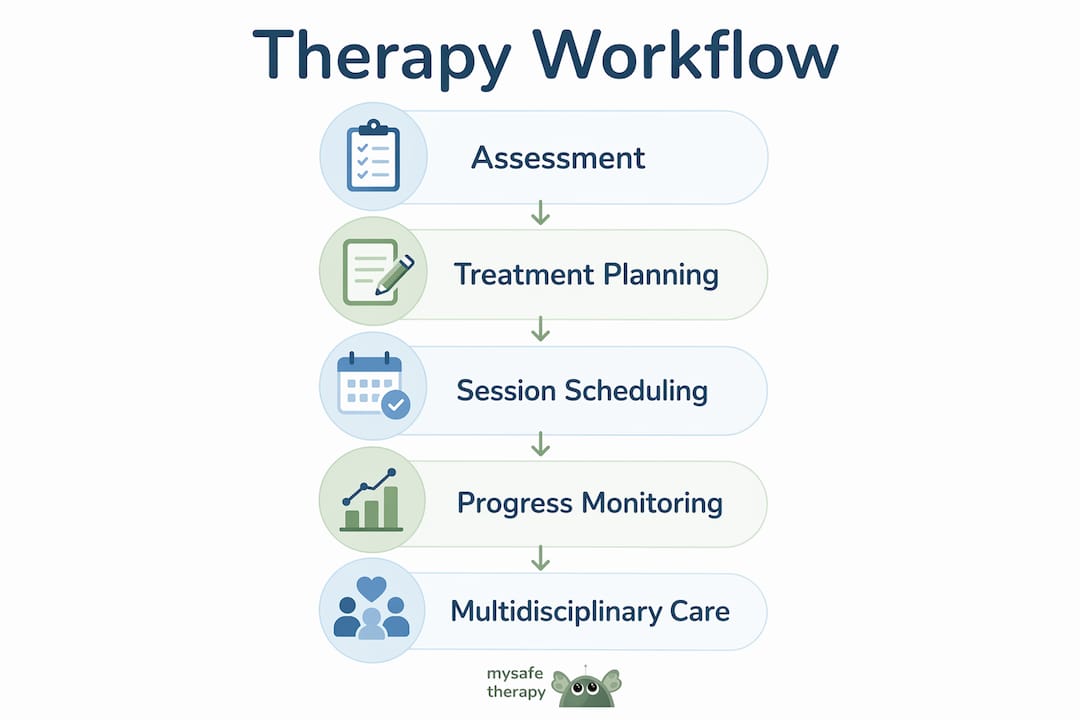
- An evidence-based therapy workflow combines research, clinical expertise, and client needs to guide treatment from assessment to discharge. It emphasizes structured assessment, protocol-driven intervention, regular outcome monitoring, and multi-agency collaboration. Proper documentation of supervision and flexibility in clinical judgment are essential for optimal outcomes.
An evidence-based therapy workflow is a structured clinical process that integrates the best available research, practitioner expertise, and individual client factors to guide treatment from assessment through to discharge. The term aligns with what the American Psychological Association and UK bodies such as BACP and NICE formally describe as evidence-based practice in psychology. For mental health practitioners in the UK, this means working within frameworks like NICE guidelines and BACP competency standards to deliver care that is both clinically sound and responsive to each client. Getting this right matters: structured workflows reduce clinical drift, support consistent outcomes, and protect both clients and practitioners.
What are the essential components of an evidence-based therapy workflow?
The foundation of any evidence-based therapy workflow is a structured assessment that determines where a client sits on the severity spectrum. The UK Stepped Care Model, mandated under NICE NG222, prescribes a four-step pathway: assessment, low-intensity intervention, high-intensity intervention, and specialist care. The model matches care intensity to clinical need, which means practitioners do not default to high-intensity therapy when guided self-help would suffice. That matching principle is what separates a structured workflow from ad hoc clinical decision-making.
Treatment planning follows directly from assessment. Once a practitioner identifies the appropriate step, the workflow specifies which intervention to deliver, at what intensity, and for how long. NICE 2026 guidelines mandate a minimum of 16 one-to-one CBT sessions for adults with psychosis, and family interventions for children and young people lasting 3–12 months. These are not suggestions. They are minimum standards that define what a clinically adequate course of treatment looks like.
Session scheduling is the third component. A well-designed workflow specifies session frequency, review points, and escalation criteria before treatment begins. This prevents the common problem of open-ended therapy with no clear endpoint or progress check.
| Intervention | Client group | Minimum duration |
|---|---|---|
| CBT (one-to-one) | Adults with psychosis | 16 sessions |
| Family intervention | Children and young people | 3–12 months |
| Low-intensity guided self-help | Mild to moderate depression | As per NICE NG222 step 2 |
| High-intensity CBT | Moderate to severe depression | As per NICE NG222 step 3 |
Pro Tip: Map every new client to a Stepped Care step at assessment and document the rationale. This single habit prevents both under-treatment and unnecessary escalation.
How can integrated care and multi-agency collaboration be incorporated into therapy workflows?
Complex clients rarely sit within a single service. A clinical workflow that ignores this reality will produce fragmented care. The reciprocal consultation model used in NHS Talking Therapies addresses this directly by building multi-agency input into the workflow itself. Triadic review sessions occur at every sixth therapy session, bringing together the therapist, the client, and a worker from a connected service such as a substance use recovery team. That interval is not arbitrary. It creates a regular checkpoint without disrupting therapeutic momentum.
Fortnightly MDT meetings extend this further by enabling joint referral review, proactive therapy initiation, and senior practitioner consultation across disciplines. These meetings serve three functions within a workflow:
- Joint care planning: All involved services agree on treatment priorities and responsibilities.
- Referral review: Cases waiting for therapy are assessed for urgency and appropriate step allocation.
- Reciprocal consultation: Senior practitioners from different disciplines advise on complex presentations without requiring formal cross-referral.
Service transformation across the UK is already moving in this direction. The BABCP has noted a shift towards community-integrated models involving multidisciplinary teams across education, NHS, and community providers to prevent crisis escalation. Practitioners who build collaboration into their workflows now are ahead of where commissioning requirements are heading.
Pro Tip: If your service does not yet hold formal MDT meetings, start with a monthly case consultation slot involving one external partner. Consistency matters more than frequency at the outset.
What tools and methods support monitoring progress and ensuring clinical competence?
Progress monitoring is not optional within a credible clinical workflow. Patient-Reported Outcome Measures, known as PROMs, provide the mechanism for detecting whether a client is improving, stalling, or deteriorating between sessions. PROMs integrated into workflows allow practitioners to identify subtle therapy stalling early, enabling timely adjustments rather than waiting until a course of treatment ends. That distinction matters clinically. A practitioner who waits for end-of-treatment data to assess progress has already lost several sessions in which a different approach might have helped.
Competency frameworks set the professional standard for who delivers these interventions and under what conditions. The BACP's Addictions Competence Framework requires three days of initial training followed by 12 monthly supervision sessions to maintain ethical and legally compliant practice. That structure reflects a broader principle: competence is not a one-time qualification but an ongoing, supervised process.
Supervision itself must be embedded in the workflow, not treated as an optional extra. The SCoPEd framework mandates that formal supervision and reflexive practice are documented for accreditation purposes. Omitting this from a workflow does not just affect quality. It puts a practitioner's registration at risk.
The monitoring and supervision cycle within a workflow follows this sequence:
- Administer PROMs at every session and score immediately.
- Review scores against expected trajectory at the midpoint of the agreed treatment length.
- Discuss cases showing no improvement or deterioration in the next scheduled supervision session.
- Document supervision content, including reflexive discussion of the practitioner's own responses to the client.
- Adjust the treatment plan formally and record the clinical rationale.
Pro Tip: Use a standardised outcome measure consistently across your caseload rather than switching tools. Consistent data allows meaningful comparison and supports your own practice-based evidence.
How to implement evidence-based therapy workflows in clinical practice
Implementation begins with prerequisites. Practitioners need access to current clinical guidelines, relevant training, and a service structure that supports structured working. UK-accredited therapists registered with BACP, UKCP, or NCPS already operate within frameworks that require evidence-based practice. The workflow formalises what good practitioners do intuitively.
The steps for adopting a structured workflow in practice are as follows. First, conduct a thorough assessment and assign the client to a Stepped Care level. Second, select the appropriate intervention and document the evidence base for that choice. Third, agree a session schedule with the client, including review points and discharge criteria. Fourth, administer PROMs from session one. Fifth, schedule supervision to coincide with review points so that clinical decisions are informed by both outcome data and reflective discussion. Sixth, document all decisions and their rationale in the clinical record.
The most common implementation pitfall is rigid manual adherence without clinical judgement. A workflow is a structure, not a script. NICE guidelines specify minimum session counts, not maximum ones. A client who reaches session 16 of CBT without sufficient progress requires a clinical decision, not automatic discharge. The three pillars of evidence-based practice are research evidence, clinical expertise, and client values. A workflow that ignores any one of these three produces worse outcomes than no workflow at all.
| Workflow model | Best suited to | Key limitation |
|---|---|---|
| Stepped Care (NICE NG222) | Depression, anxiety in primary care | Requires clear severity thresholds at assessment |
| Reciprocal consultation model | Complex cases with co-occurring conditions | Needs established inter-agency relationships |
| Practice Research Network model | Services seeking to generate local evidence | Requires research infrastructure and governance |
| Competency-based supervision model | Specialist or addictions services | Time-intensive for supervisors |
Scheduling therapy sessions in a structured way is itself a workflow decision. Irregular or client-led scheduling without clinical rationale undermines the treatment plan. Session frequency should be determined by the intervention protocol, not by client or practitioner convenience alone.
The disconnect between research and real-world practice is the most persistent challenge in this field. Practice Research Networks address this by generating evidence under actual clinical service conditions. The UK Northern Talking Therapies PRN published over 20 studies in 10 years, each one improving real-world therapy workflows in ways that randomised controlled trials cannot replicate. Connecting your service to a PRN is one of the most practical steps a practitioner or service lead can take.
Key takeaways
An effective evidence-based therapy workflow requires structured assessment, protocol-driven session planning, integrated multi-agency collaboration, routine outcome monitoring, and documented clinical supervision.
| Point | Details |
|---|---|
| Stepped Care is the foundation | Match intervention intensity to severity using the NICE NG222 four-step model from the outset. |
| Session counts are minimum standards | NICE mandates at least 16 CBT sessions for adult psychosis; treat this as a floor, not a ceiling. |
| Multi-agency reviews prevent fragmentation | Build triadic reviews at every sixth session into the workflow for complex or co-occurring presentations. |
| PROMs detect stalling early | Administer outcome measures every session and act on the data before the course of treatment ends. |
| Supervision protects registration | Document formal supervision and reflexive practice to meet SCoPEd accreditation requirements. |
Why workflows need more than a manual
Working with evidence-based therapy for any length of time makes one thing clear: the practitioners who deliver the best outcomes are not those who follow protocols most rigidly. They are the ones who understand why each protocol element exists and exercise clinical judgement when the evidence and the client in front of them do not align neatly.
The "three-legged stool" framing of evidence-based practice is useful precisely because it resists the temptation to treat research as the only authority. A NICE guideline tells you what works on average across a population. It does not tell you what this client needs in this session. Clinical expertise and client values fill that gap. Practitioners who treat workflows as a substitute for thinking will eventually produce harm, even when following guidance to the letter.
The gap between research and practice is real and persistent. Practice Research Networks exist because randomised controlled trials, however rigorous, are conducted under conditions that rarely match a community mental health service on a Tuesday afternoon. The UK Northern Talking Therapies PRN model shows that services can generate their own meaningful evidence without academic infrastructure. That is the kind of practice-based evidence that actually changes how practitioners work day to day.
Supervision is the element most often treated as administrative rather than clinical. That is a mistake. Reflexive supervision is where practitioners process the emotional weight of complex cases, identify their own blind spots, and maintain the quality of their clinical judgement over time. A workflow that does not protect supervision time will eventually produce burnout and clinical drift, regardless of how well-designed the rest of the process is.
— Mysafetherapy
Therapy for professionals: how Mysafetherapy supports your practice
Mental health practitioners carry the same pressures they help clients address, and structured support makes a measurable difference to clinical quality and personal well-being.
Mysafetherapy connects practitioners with therapy for professionals delivered by UK-accredited therapists registered with BACP, UKCP, and NCPS. Sessions are available via video, chat, or avatar format, including evenings and weekends, so access fits around clinical commitments. All therapists on the platform work within evidence-based frameworks, and the service maintains full transparency on therapist standards and accreditation. Whether you are looking for personal support or a structured space to reflect on your practice, Mysafetherapy offers confidential, affordable access without waiting lists.
FAQ
What is an evidence-based therapy workflow?
An evidence-based therapy workflow is a structured clinical process that combines research evidence, practitioner expertise, and client values to guide assessment, treatment planning, session delivery, and outcome monitoring from referral to discharge.
How many CBT sessions does NICE recommend for adult psychosis?
NICE 2026 guidelines specify a minimum of 16 one-to-one CBT sessions for adults with psychosis. This is a minimum standard, not a fixed course length.
What are PROMs and why do they matter in therapy workflows?
Patient-Reported Outcome Measures are standardised questionnaires completed by clients to track their progress. Integrating PROMs into every session allows practitioners to detect therapy stalling early and adjust treatment before the course ends.
How does the Stepped Care Model work in UK mental health services?
The Stepped Care Model, mandated under NICE NG222, assigns clients to one of four levels of care based on severity: assessment, low-intensity, high-intensity, and specialist. The least intrusive effective intervention is always offered first.
What happens if supervision is not documented in a therapy workflow?
Omitting documented supervision and reflexive practice from a workflow puts a practitioner's accreditation at risk under the SCoPEd framework. Supervision is a mandatory workflow element, not an optional professional development activity.