
TL;DR:
- Blended therapy combines face-to-face psychotherapy with digital tools to improve accessibility, flexibility, and effectiveness. It involves a single clinician tailoring the balance of in-person and digital support, offering benefits like shorter treatments and reduced dropout rates. This approach is increasingly integrated into NHS services and private practices, emphasizing ongoing digital engagement supervised by trained therapists.
Many people assume blended therapy is simply a polished way of saying "online therapy." That assumption misses the point entirely. What is blended therapy, properly understood, is a clinical model that deliberately combines face-to-face psychotherapy with self-guided digital tools to create treatment that is more flexible, more accessible, and often more effective than either approach alone. This article explains how blended therapy works, what the research says about its outcomes, and how the NHS and private providers are putting it into practice across the UK.
Table of Contents
- Key takeaways
- What is blended therapy?
- Benefits of blended therapy
- Challenges in delivering blended therapy
- Types of blended therapy techniques
- Blended therapy in NHS and private practice
- My perspective on blended therapy
- Start blended therapy with Mysafetherapy
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Not a replacement for in-person care | Blended therapy combines digital and face-to-face methods rather than substituting one for the other. |
| Clinically significant outcomes | PHQ-9 depression scores and GAD-7 anxiety scores show marked improvements sustained at one-year follow-up. |
| Shorter treatment durations | NHS blended models show treatment periods up to 121 days shorter than standard stepped care pathways. |
| Therapist involvement is critical | Digital tools work best when therapists actively prescribe and review them during live sessions. |
| Accessible for more people | Blended formats remove barriers related to location, working hours, and caring responsibilities. |
What is blended therapy?
Blended therapy integrates face-to-face psychotherapy with self-guided digital health interventions, such as CBT modules, app-based exercises, mood trackers, and psychoeducation resources, into a single coordinated treatment plan. The defining feature is that both components run simultaneously, overseen by a single therapist who tailors the balance to each patient's needs.
This distinguishes blended therapy from two models it is often confused with.
- Online therapy replaces face-to-face contact with video or chat sessions but does not necessarily involve self-guided digital tools between appointments.
- Stepped care moves patients sequentially from lower-intensity digital support to higher-intensity in-person therapy if the first step does not work. Blended therapy, by contrast, adjusts treatment intensity in real time rather than waiting for one level to fail before escalating.
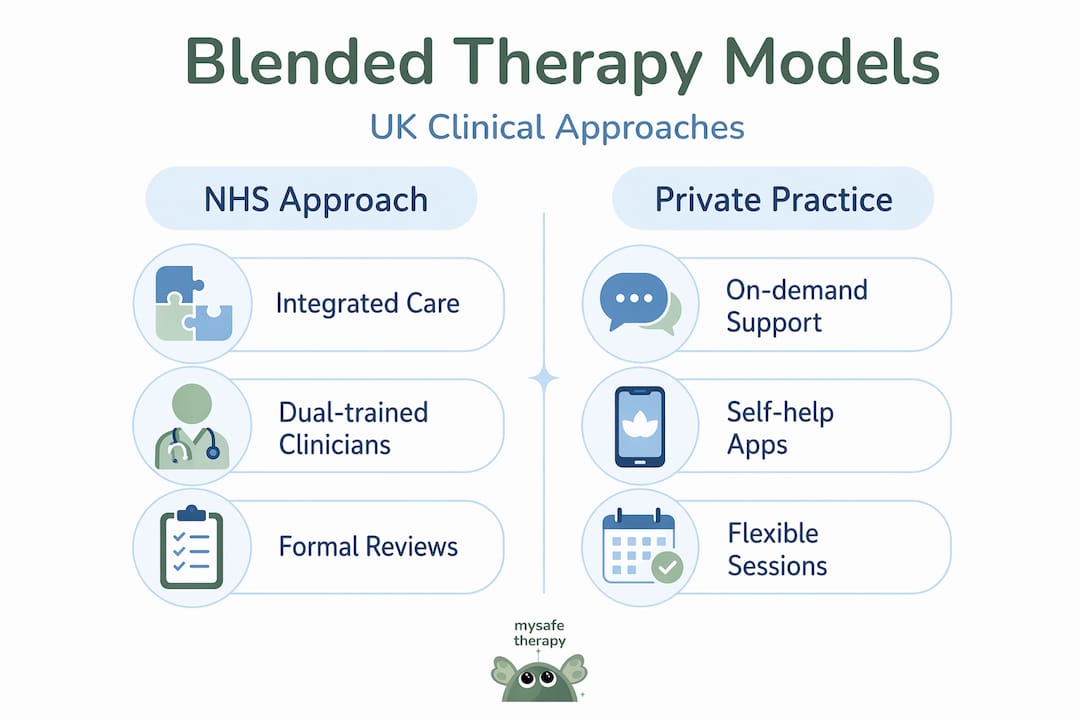
Within the blended therapy category, three broad models are common in UK practice.
| Model | Description | Typical use |
|---|---|---|
| Integrative blended | Digital and in-person elements are tightly woven together by one clinician | Anxiety, depression, trauma |
| Sequential blended | Digital tools are introduced at specific stages alongside sessions | Structured CBT programmes |
| Complementary blended | Digital resources supplement sessions without being formally prescribed | Psychoeducation, mood tracking |
The integrative model is the most clinically rigorous and is what the NHS Talking Therapies programme is working towards. It requires what researchers call a dual-trained clinician, someone trained in both low-intensity and high-intensity CBT, who can move between digital and in-person elements without handing the patient between services.
Benefits of blended therapy
The clinical case for blended therapy is not theoretical. Patients receiving a structured blended CBT intervention for depression in primary care showed PHQ-9 scores drop from 16 to 6 and GAD-7 anxiety scores fall from 14 to 5. Those improvements were maintained at 52-week follow-up, which is a result that purely digital self-help tools rarely replicate on their own.
Beyond symptom reduction, the practical benefits of blended therapy are substantial.
- Reduced dropout. Engagement with digital-only mental health tools is inconsistent, with dropout rates ranging from 15% to 65%. Adding regular human contact from a therapist significantly reduces disengagement.
- Fewer missed appointments. When patients can complete exercises digitally between sessions, they come to live appointments better prepared and more engaged, which translates to fewer cancellations.
- Shorter treatment durations. The NHS Talking Therapies blended model produced treatment periods 121 days shorter than standard stepped care on average.
- Patient empowerment. Self-guided modules give people skills and tools they can use independently, which builds confidence between sessions.
- Greater accessibility. Blended therapy helps patients with caring responsibilities, those living in rural areas, and people with demanding work schedules access treatment they might otherwise go without.
Pro Tip: If you are comparing therapy options, ask directly whether digital tasks are formally reviewed in sessions or simply recommended. The former is blended therapy. The latter is standard therapy with an app attached.
Challenges in delivering blended therapy
Blended therapy is not without its complications, and it is worth understanding them before committing to a programme.
The first is the digital-human disconnect. Some patients engage readily with digital modules between sessions; others barely open them. When engagement drops, the therapist needs to address it directly rather than allowing the digital component to become background noise. Blended therapy does not replace the therapeutic relationship. It extends it via digital tools, providing ongoing support between sessions. If that extension breaks down, the model loses much of its advantage.

Measuring dropout is another genuine complexity. Patients can disengage from the digital component, the in-person sessions, or both, and these patterns carry different clinical meanings. Researchers recommend reporting dropout rates separately for digital and in-person components, but many services do not yet do this, making it hard to compare outcomes across providers.
There are operational pressures on clinicians too. Managing a dual-intensity caseload requires ongoing coordination, and training staff to work fluidly across both modalities takes time and resource that not every service can afford. Understanding technology's role in therapy helps clinicians frame digital tools correctly from the outset, rather than treating them as optional extras.
Pro Tip: When starting blended therapy, ask your therapist how digital tasks will be reviewed in sessions. Clear expectations from the start reduce the risk of disengaging from the digital component without realising it.
Types of blended therapy techniques
The techniques used in blended therapy draw from several well-established therapeutic traditions. What makes them "blended" is how they are delivered and coordinated, not the techniques themselves.
- CBT modules via apps or online platforms. Cognitive behavioural therapy is the most commonly used approach in blended formats. Patients complete thought records, behavioural activation schedules, and psychoeducation between sessions, then review them with their therapist.
- Psychoeducation resources. Written or video-based materials help patients understand their diagnosis, how their symptoms develop, and what maintains them. This provides context that makes in-session work more productive.
- Mood and symptom tracking. Smartphone apps that log daily mood, sleep, or anxiety levels give therapists real data to work with and help patients notice patterns they would otherwise miss.
- Thought-challenging exercises. Structured worksheets or app prompts guide patients through identifying and reframing unhelpful thought patterns between sessions.
- Narrative and emotion-focused techniques. For patients dealing with relational difficulties or complex family situations, narrative therapy and Emotionally Focused Therapy can be integrated into blended programmes to address the relational and emotional dimensions of mental health.
- Homework and skills assignments. Therapists prescribe specific tasks aligned to the session content. Patients using therapist-prescribed digital assignments consistently show higher engagement and better outcomes than those using apps independently.
Therapists working in personalised therapy models tailor these components individually, selecting the right techniques for each patient's presentation rather than applying a fixed protocol to everyone.
Blended therapy in NHS and private practice
The NHS Talking Therapies programme has moved furthest in formalising blended therapy in the UK. Under their model, dual-trained clinicians manage both low-intensity digital-based support and high-intensity face-to-face CBT for the same patient, adjusting the balance as the patient's needs change. Preliminary evaluation data shows this approach produces outcomes comparable to traditional stepped care but with meaningfully shorter treatment durations and fewer missed appointments.
Patient journeys through NHS blended therapy often follow a recognisable pattern. A patient presenting with moderate depression might begin with two or three structured face-to-face sessions, then shift to a mix of fortnightly sessions and weekly app-based exercises, with the therapist reviewing progress and adjusting the digital component at each appointment. This flexibility is particularly valuable for people whose circumstances change during treatment.
Key access considerations in the UK context include:
- People in rural areas who face long travel times to therapy centres benefit from reduced in-person session frequency.
- Those with full-time employment or caring responsibilities can complete digital elements at evenings or weekends without waiting for appointment slots.
- Patients who find the formality of repeated face-to-face contact anxiety-provoking often respond well to a lighter in-person schedule supported by digital tools.
In the private sector, platforms offering self-help resources for flexible support alongside live therapy are filling gaps where NHS waiting times remain long. The distinction between a genuinely blended model and a platform that simply offers both video sessions and an app matters considerably. The clinical value comes from integration and therapist oversight, not from the existence of both formats side by side.
My perspective on blended therapy
I've worked closely enough with this model to say something that most overviews skip. Blended therapy is not an upgrade to traditional therapy. It is a redesign of the therapeutic process itself.
The real shift is in what happens between sessions. Traditional therapy asks patients to remember insights and apply them independently until the next appointment. Blended therapy creates a structured environment where the work continues through digital tools that are directly tied to session content. That continuity is where much of the clinical benefit comes from.
What I've seen consistently is that the therapist's involvement in prescribing and reviewing digital tasks is the single most important variable. When therapists treat digital modules as mandatory and clinically significant, patients treat them the same way. When therapists mention them as optional extras, patients ignore them. The availability of dual-trained clinicians is what makes this possible at scale, but it requires services to invest in training that many have not yet prioritised.
The patients who benefit most are those who want to do the work but need structure to do it. Blended therapy provides that structure without overwhelming people with appointments. Done well, it makes therapy fit around a person's life rather than the other way around.
— MySafeTherapy
Start blended therapy with Mysafetherapy
Mysafetherapy connects you with UK-accredited therapists registered with professional bodies including BACP, UKCP, and NCPS, offering a model that combines live sessions with structured digital support between appointments.
Every therapist on the platform is individually matched to your needs, and sessions are available via video, chat, or avatar-based formats to suit your preference and schedule, including evenings and weekends. Whether you are managing anxiety, depression, burnout, or relationship difficulties, you can start therapy online with a therapist who understands how to integrate digital tools meaningfully into your treatment. Flexible scheduling, transparent pricing, and easy therapist switching mean the process works around your life, not against it. Confidentiality is built into every step.
FAQ
What is blended therapy and how does it differ from online therapy?
Blended therapy combines face-to-face psychotherapy with self-guided digital tools into one coordinated treatment plan. Online therapy replaces in-person sessions with video or chat but does not necessarily involve structured digital work between appointments.
Is blended therapy effective for anxiety and depression?
Yes. Research shows that blended CBT produces clinically significant reductions in both depression and anxiety scores, with PHQ-9 scores dropping from 16 to 6 and GAD-7 scores from 14 to 5, with gains maintained at one-year follow-up.
How does blended therapy work in the NHS?
NHS Talking Therapies uses dual-trained clinicians to deliver both low-intensity digital support and high-intensity face-to-face CBT within a single treatment pathway, adjusting the balance as the patient's needs evolve.
What types of blended therapy techniques are commonly used?
Common techniques include app-based CBT modules, mood and symptom tracking, psychoeducation resources, thought-challenging worksheets, and therapist-prescribed digital homework reviewed during live sessions.
How do I know if blended therapy is right for me?
Blended therapy suits people who want structured support between sessions and need flexibility around work, location, or caring responsibilities. Speaking with a qualified therapist about your circumstances is the most reliable way to assess whether the model fits your needs.