
TL;DR:
- Trauma therapy is an evidence-based approach that helps process distressing experiences without forcing detailed recounting. It aims to reduce emotional intensity attached to memories, promoting healing through safety and consistency. Prompt, supported intervention can improve recovery, with therapies like EMDR and CPT tailored to individual needs.
Many people searching for what is trauma therapy are working from a fundamental misconception: that sitting in a therapist's office means being required to recount every painful detail of what happened to them. This assumption stops a significant number of people from ever making that first appointment. Trauma therapy is a structured, evidence-based form of psychological treatment designed to help people process distressing experiences that have overwhelmed their ability to cope. It is not about forcing you to relive the past. It is about helping your brain finally make sense of it.
Table of Contents
- Key takeaways
- Understanding trauma and how it affects you
- Main types of trauma therapy used in the UK
- When to seek trauma therapy
- Common myths about trauma therapy
- Practical steps to begin trauma therapy
- My perspective on trauma therapy
- Start trauma therapy with Mysafetherapy
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Trauma therapy is evidence-based | Methods like trauma-focused CBT and EMDR are clinically proven and recommended by the NHS for adults with PTSD. |
| Reliving trauma is not required | Therapies such as CPT and EMDR process trauma without forcing detailed verbal recounting of events. |
| Timing matters | Waiting at least four weeks after a traumatic event before starting trauma-focused therapy is generally advisable. |
| Consistency drives recovery | Weekly sessions with the same therapist build the safety and trust necessary for genuine healing. |
| Therapy reprocesses, not erases | The goal is to reduce emotional intensity attached to memories, not to remove them from your mind. |
Understanding trauma and how it affects you
Trauma is not simply a bad experience. It is what happens when an experience overwhelms your capacity to process and integrate it. In the UK, common causes include road traffic accidents, physical or sexual assault, childhood abuse, sudden bereavement, domestic violence, and witnessing violence. Medical emergencies and the aftermath of serious illness also feature prominently, as do experiences tied to military service.
Psychologists distinguish between two broad categories. Single-incident trauma, sometimes called Type I, refers to one discrete event such as a car accident or assault. Complex trauma, or Type II, involves repeated or prolonged exposure to distressing events, often beginning in childhood. The two require somewhat different therapeutic approaches, though they share many of the same evidence-based methods.
What makes trauma particularly disruptive is what it does to the brain. Under extreme stress, the brain's threat-detection system takes over and prioritises survival above everything else. This means fragmented, jumbled memories are stored rather than coherent narratives. When something in the present environment triggers those incomplete memories, the brain responds as though the danger is happening right now. The body follows: heart rate rises, muscles tense, breathing changes.
Common symptoms experienced by adults include:
- Intrusive memories, flashbacks, or nightmares
- Avoidance of people, places, or situations linked to the trauma
- Emotional numbness or feeling detached from others
- Hypervigilance and an exaggerated startle response
- Difficulty concentrating, sleeping, or experiencing positive emotions
- Physical symptoms such as headaches, fatigue, or digestive problems
The critical point here is that avoidance behaviours prevent the brain from completing its natural processing of what happened, which is precisely why professional support becomes necessary for many people.
Main types of trauma therapy used in the UK
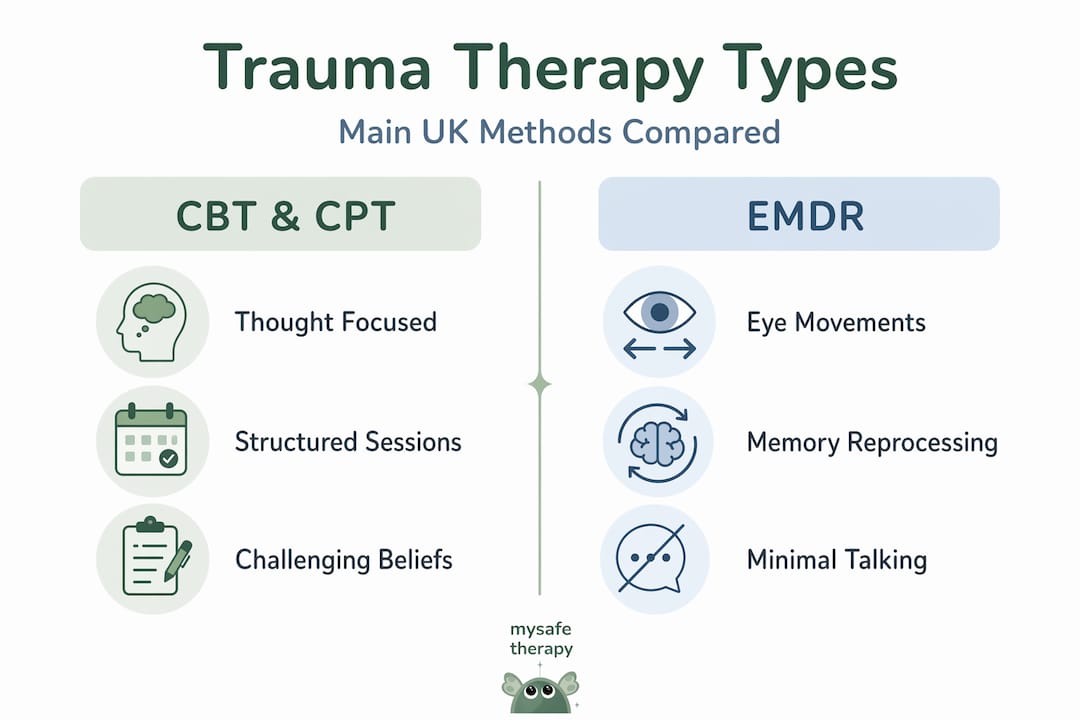
The primary evidence-based therapies recommended for adults with PTSD in the UK are trauma-focused cognitive behavioural therapy (TF-CBT) and Eye Movement Desensitisation and Reprocessing (EMDR). A third approach, Cognitive Processing Therapy (CPT), is also widely used and particularly well-suited to people who struggle with verbalising their experiences.
| Therapy | How it works | Best suited for |
|---|---|---|
| Trauma-focused CBT | Identifies and challenges unhelpful thoughts linked to the trauma | Single-incident and complex trauma |
| EMDR | Uses bilateral stimulation (eye movements or tapping) to reprocess traumatic memories | PTSD, phobias, and complex trauma |
| CPT | Challenges distorted beliefs about the trauma without requiring full verbal recounting | Those who find talking in detail difficult |
Trauma-focused CBT works by helping you identify the thoughts and beliefs that formed in the aftermath of trauma. These are often distorted: "I should have done something", "It was my fault", "Nowhere is safe." The therapist guides you to examine these beliefs against evidence, gradually reducing their grip. Sessions typically involve some structured exposure to trauma-related material, but this is paced carefully and never without your consent.
EMDR often surprises people. Rather than spending sessions talking through the trauma in chronological order, you are guided to hold a specific memory in mind while the therapist introduces bilateral stimulation, usually through guided eye movements. This process appears to help the brain reprocess the stored memory so it loses its raw emotional charge. It is one of the most widely studied trauma therapies in existence.
CPT is particularly notable because it was designed to process trauma without requiring detailed verbal recounting. Instead, it focuses on the meaning you have assigned to the traumatic event and the stuck points in your thinking. For people who find talking through what happened deeply distressing, this can be a more accessible starting point.
Per NHS and NICE guidance, adults typically receive 8 to 12 weekly sessions of trauma-focused therapy, each lasting 60 to 90 minutes. These sessions are not casual conversations. They are structured, purposeful, and follow a clinical framework.
Pro Tip: When researching therapists, look specifically for those trained in trauma-focused methods rather than general counsellors. The distinction matters. Not all talking therapies are designed for trauma, and working with a trauma-trained clinician significantly affects outcomes. You can read more about evidence-based therapy methods recommended by healthcare authorities.
When to seek trauma therapy
One of the most common questions people ask is simply: when? Not everyone who experiences a traumatic event will go on to develop PTSD or require formal therapy. Many people recover naturally within a few weeks as the brain gradually processes what happened.
Here is a practical framework for thinking through the timing:
- Give yourself space initially. Difficult feelings often improve naturally within days or weeks after a traumatic event. This is your brain doing what it is designed to do.
- Monitor your symptoms over the first month. If intrusive thoughts, nightmares, or avoidance behaviours are persisting or worsening rather than easing, this is a clear signal that additional support is warranted.
- Wait before beginning trauma-focused therapy. Waiting at least four weeks after the traumatic event before commencing trauma-focused therapy is generally recommended. Starting too early can sometimes interfere with the brain's natural processing.
- Seek assessment if symptoms persist beyond one month. At this point, a formal assessment from a trained clinician helps determine the most appropriate course of action.
- Do not delay indefinitely. Avoidance is one of the most common barriers to recovery. If you are unsure whether you need support, an honest self-assessment is a useful first step. The do I need therapy quiz from Mysafetherapy can help clarify this.
Pro Tip: Avoid seeking trauma-focused therapy as a single isolated session. Trauma processing requires continuity. A one-off appointment can sometimes feel more destabilising than helpful if it opens difficult material without the safety net of an ongoing therapeutic relationship.
Common myths about trauma therapy
Misconceptions about trauma therapy are widespread, and they cause real harm by keeping people from accessing support they need. The shift that trauma-informed therapy represents is profound: as one framework puts it, the focus moves from "what's wrong with you?" to "what happened to you?" That is a fundamentally different kind of conversation.
Here are the most persistent myths, and what the evidence actually shows:
- Myth: You have to recount every detail of what happened. In reality, therapies such as CPT and EMDR are specifically designed to process trauma without forcing full verbal recounting. Your pace and comfort are central to the process.
- Myth: Therapy will erase your memories. The goal of trauma therapy is not deletion. It is reprocessing. A well-delivered course of therapy helps the brain reduce emotional intensity attached to memories, so they no longer feel like present-tense threats.
- Myth: Medication is the most effective first step. Medication is not offered as first-line treatment for adult PTSD. Psychological therapy is the primary recommendation. Medication may be used alongside therapy in specific cases, but it is not the starting point.
- Myth: Trauma therapy follows a single template. Effective trauma therapy is personalised. The approach, pacing, and techniques are adjusted to fit your specific history, symptoms, and preferences.
"Trauma therapy works not by forcing you back into the worst moments of your life, but by creating enough safety that your mind can finally process what it could not process at the time."
This reframing matters. The therapy room is not where you go to suffer through the past again. It is where you learn that the past no longer has to control the present.
Practical steps to begin trauma therapy
Knowing the theory is one thing. Taking the first practical steps is another. Here is how to approach this with clarity:
- Find a trauma-trained therapist. Look for UK-accredited therapists registered with professional bodies such as the BACP, UKCP, or NCPS who hold specific training in trauma-focused methods. General counselling experience is not equivalent.
- Know what to expect from early sessions. Initial sessions focus on assessment and building a therapeutic relationship. You will not be asked to process traumatic material immediately. Safety comes first.
- Prioritise consistency. Weekly sessions with the same therapist are not a preference, they are a clinical requirement for effective trauma healing. The relationship itself is part of the treatment.
- Support yourself between sessions. Trauma processing can surface difficult feelings. Mental health management strategies such as grounding exercises, sleep hygiene, and physical movement help stabilise your experience between appointments.
- Prepare emotionally rather than intellectually. Many people spend time rehearsing what they will say to a therapist. This is not necessary. What matters more is being open to the process, even when it feels uncertain.
The clinical evidence is clear that trauma-focused therapy, delivered by trained therapists, is the most effective available approach. What it requires from you is consistency and the willingness to engage, not perfection or readiness.
My perspective on trauma therapy
I've worked closely with the topic of trauma therapy long enough to have formed some firm views. The single biggest barrier I've observed is not fear of the therapy itself. It is the story people tell themselves about what therapy will demand of them.
People arrive believing they will have to relive the worst moment of their life in graphic detail, week after week, until they have somehow exhausted it. That belief is wrong, and it keeps people suffering unnecessarily. What I've learned is that effective trauma therapy is far more about creating safety than revisiting pain.
The therapist-client relationship is not incidental to trauma healing. It is the mechanism. When someone has experienced trauma, their nervous system has learned that the world is not safe. A consistent, predictable, non-judgmental therapeutic relationship begins to contradict that learning at a neurological level. This is why the guidance to see the same therapist weekly is not just procedural. It is foundational.
I've also noticed that the people who resist starting therapy the longest are often the ones who benefit from it most. Avoidance feels protective. It is actually prolonging the problem. My honest view: do not wait until you feel ready. Readiness tends to follow action, not precede it.
— MySafeTherapy
Start trauma therapy with Mysafetherapy
If you are ready to take the next step, Mysafetherapy connects you with UK-accredited therapists who are specifically trained in trauma-focused methods, including TF-CBT and EMDR, and registered with professional bodies such as BACP, UKCP, and NCPS.
Sessions are available online via video, chat, or avatar formats, so you can access support from home, on your schedule, including evenings and weekends. All therapists on the platform work in line with NICE guidelines, meaning your care is grounded in the same clinical standards that apply across the NHS. Pricing is transparent, sessions are confidential, and switching therapists is straightforward if your needs change. To take the first step, start therapy today with a therapist matched to your specific needs.
FAQ
What is trauma therapy and who is it for?
Trauma therapy is a structured, evidence-based psychological treatment designed to help people process and recover from traumatic experiences. It is suitable for any adult experiencing persistent distress after a traumatic event, whether that is a single incident or prolonged exposure over time.
How does trauma therapy work?
Trauma therapy uses techniques such as TF-CBT, EMDR, and CPT to help the brain reprocess traumatic memories, reducing their emotional intensity and allowing the person to function without being triggered by past events.
Do I have to relive the trauma in detail during sessions?
No. Therapies such as CPT and EMDR are specifically designed to process traumatic experiences without requiring full verbal recounting of events. The pace and approach are always adjusted to what you can manage safely.
How many trauma therapy sessions will I need?
Per NHS and NICE guidance, most adults with PTSD receive 8 to 12 weekly sessions of trauma-focused therapy, each lasting 60 to 90 minutes. Some people may need fewer or more sessions depending on the nature and complexity of their trauma.
When should I start trauma therapy after a traumatic event?
It is generally advisable to wait at least four weeks after a traumatic event before beginning formal trauma-focused therapy, allowing time for natural processing. If symptoms persist or worsen beyond one month, seeking a clinical assessment is recommended.