TL;DR:
- Mental health stigma persists in the UK despite increased awareness, and therapy actively disrupts this cycle by providing acceptance, psychoeducation, and social contact. Specific therapeutic mechanisms, especially group formats and online options, effectively reduce internalised shame and barriers to help-seeking. However, outcomes vary, requiring informed choices and targeted approaches to address ongoing social and structural challenges.
Mental health stigma persists in the UK despite a decade of growing public awareness and increased access to support services. Stigma-related knowledge and behaviours are measurably improving, yet many people still delay or avoid seeking help because of internal shame or fear of others' reactions. Therapy, it turns out, does more than address symptoms. It actively disrupts the cycle of stigma itself. This article explains the precise mechanisms by which therapy reduces mental health stigma, what the UK evidence shows, and what this means for anyone considering taking that first step.
Table of Contents
- Understanding stigma: barriers to seeking help
- Mechanisms: how therapy directly counters stigma
- Evidence from the UK: programmes, therapy, and changing attitudes
- Challenges and what still needs work
- What most articles miss about therapy and mental health stigma
- Find accessible therapy to break the stigma
- Frequently asked questions
Key Takeaways
| Point | Details |
|---|---|
| Therapy normalises support | Modern therapy makes seeking help socially acceptable in the UK, challenging old stereotypes. |
| Social contact is crucial | Interacting with others who share their experiences, especially through group therapy, helps reduce stigma. |
| Accessible formats reduce barriers | Online and flexible therapy options make it easier to seek support without fear of judgement. |
| Stigma reduction is not automatic | Therapy helps most people, but individual experiences with stigma vary depending on context and issue. |
Understanding stigma: barriers to seeking help
Stigma in the context of mental health takes two distinct forms. Public stigma refers to the negative attitudes held by society at large. Self-stigma, sometimes called internalised stigma, is what happens when a person absorbs those external beliefs and begins to apply them to themselves. Both are harmful, but self-stigma is often harder to identify and more directly responsible for preventing people from seeking help.
Common fears that prevent help-seeking include:
- Being labelled as "weak" or "unstable" by family, friends, or employers
- Losing control over personal decisions, particularly around employment or parenting
- Being seen by others while entering a therapy clinic or mental health service
- Feeling that one's experiences are not "serious enough" to warrant professional support
- Shame about not being able to manage independently
These fears are not irrational. They reflect real social consequences that many UK adults face. Research confirms that internalised stigma reduces willingness to seek help, and this effect is particularly pronounced when the problem involves suicidal thinking. In other words, the more serious a person's distress, the more shame may silence them.
The relationship between internalised stigma and help-seeking is well documented. Self-stigma essentially acts as a filter, causing a person to pre-judge their own worthiness for care before they have even contacted a service.
"The most significant barrier to mental health support is often not the cost or availability of services. It is the internal voice telling someone they do not deserve help."
This is precisely why understanding stigma as a mechanism matters. Addressing the symptom, such as anxiety or depression, without addressing the stigma that surrounds it often leads to incomplete outcomes and, in some cases, early dropout from treatment.
Mechanisms: how therapy directly counters stigma
Understanding how stigma operates helps clarify why therapy is one of the most effective tools for reducing it. The process is not passive. Stigma reduction through therapy requires specific approaches and, in many cases, deliberate focus from the therapist.
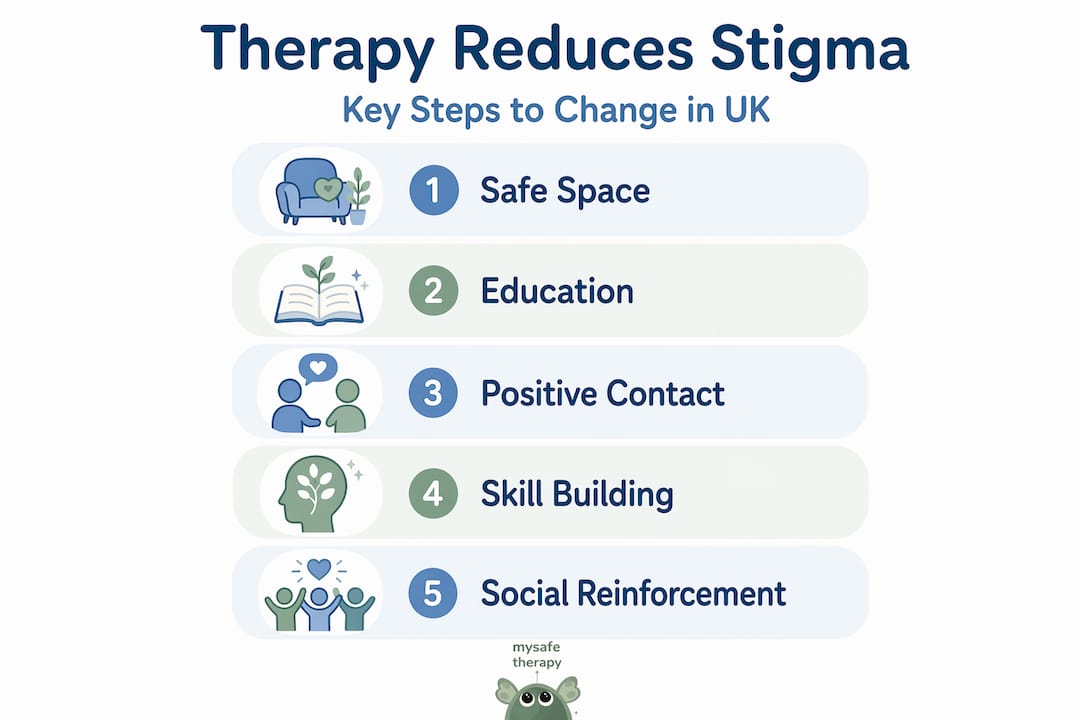
The core mechanisms through which therapy counters stigma include:
- Providing a non-judgmental relationship. For many clients, the therapeutic relationship is the first context in which they experience complete acceptance. This directly challenges the expectation of rejection that underpins self-stigma.
- Psychoeducation. Therapists provide factual information about mental health conditions, correcting distorted beliefs. Understanding that anxiety is a neurological response rather than a character flaw fundamentally changes how a person relates to their own diagnosis.
- Cognitive restructuring. Evidence-based approaches such as Cognitive Behavioural Therapy (CBT) target the specific thought patterns that sustain internalised stigma. Clients learn to identify and challenge self-critical beliefs about their mental health.
- Skills training. Practical tools for managing symptoms reduce dependence and increase confidence, which directly counteracts the sense of helplessness that stigma creates.
- Shared experience and social contact. Group therapy and peer support mechanisms allow individuals to hear stories from others with similar experiences, which humanises mental health struggles and disrupts stereotyping.
Research supports these mechanisms directly. Non-judgmental care, education, and skills training are confirmed as core clinical tools for countering the labels that stigma attaches to mental health conditions.
The social contact element deserves particular attention. Social contact theory suggests that direct, positive interaction between people with and without a given characteristic reduces prejudice. In the context of therapy, this translates to group formats where participants discover commonality rather than difference. It also applies to the therapist-client relationship when therapists share carefully chosen elements of their own experience or demonstrate understanding of stigma's effects.
| Therapy mechanism | How it reduces stigma | Evidence base |
|---|---|---|
| Non-judgmental space | Directly challenges fear of rejection | Clinical research on therapeutic alliance |
| Psychoeducation | Corrects factual misunderstandings about mental health | CBT and psychoeducation trials |
| Cognitive restructuring | Targets internalised shame beliefs | CBT outcome studies |
| Group therapy and peer contact | Applies social contact theory | Social psychology and group therapy research |
| Skills and confidence building | Reduces sense of incapacity linked to stigma | Behavioural activation studies |
Learning how therapy supports well-being reveals that these mechanisms operate in parallel rather than in sequence. A client may experience normalisation and cognitive shifts in the same session.
Pro Tip: If you are worried about being judged before you even begin therapy, raise this directly with your therapist in the first session. Trained therapists expect this concern and will address it explicitly. It is a common starting point, not an obstacle.
Accessing self-help therapy resources alongside live therapy can also reinforce these mechanisms between sessions, particularly when structured around psychoeducation and normalisation.
Evidence from the UK: programmes, therapy, and changing attitudes
The UK has invested significantly in anti-stigma programmes over the past two decades. The Time to Change campaign, which ran from 2007 to 2021, was one of the largest mental health anti-stigma programmes globally. It combined public education, lived experience storytelling, and social contact initiatives to shift attitudes across England and Wales.
The data from that period and subsequent research presents an informative picture.
- Public attitudes towards people with mental health conditions improved measurably across multiple surveys during the Time to Change era
- Willingness to discuss mental health openly increased among adults aged 18 to 64
- Discrimination reported by people with lived experience of mental illness showed a statistically significant decline
- Anti-stigma interventions combining education and lived experience produce measurable improvements in attitudes, including among health professionals who may previously have held stigmatising views
- NHS talking therapies have been redesigned to be highly accessible through online and self-referral options, directly reducing the practical and social barriers to seeking help
| Therapy delivery format | Stigma-related barrier reduced | Accessibility advantage |
|---|---|---|
| Traditional in-person therapy | Moderate, limited by visibility concerns | Lower, requires travel and scheduling |
| NHS talking therapies (self-referral) | High, removes gatekeeping | High, available without GP referral |
| Online therapy (video or chat) | Very high, removes visibility and travel concerns | Very high, evening and weekend availability |
| Group therapy | Very high, adds social contact mechanism | Moderate, varies by provider |
The shift towards online formats is particularly significant. Many people who would not enter a physical clinic will engage with therapy via video or chat. The absence of a visible waiting room, the flexibility of scheduling outside working hours, and the privacy of engaging from home all reduce the situational exposure that public stigma relies upon. This is not a compromise on quality. It is a structural redesign that directly addresses stigma as a barrier.
Support from UK therapists is now available through a wider range of formats than at any previous point, and the evidence base for their effectiveness continues to grow. Learning about the range of therapy formats available can help individuals identify the option that best fits their personal circumstances and comfort level.
Challenges and what still needs work
The evidence for therapy as a tool for stigma reduction is compelling, but it is not without limits. Results vary. Progress is not guaranteed. Understanding these limitations helps set realistic expectations and makes it easier to navigate towards the approaches most likely to help.
Key challenges include:
- Variable outcomes by problem type. Stigma intervention effects are heterogeneous, meaning what works for anxiety may not work as effectively for conditions carrying heavier social stigma, such as psychosis or substance misuse.
- Suicidal ideation remains a specific challenge. Internalised stigma and help-seeking for suicidal thoughts are linked in ways that require specialist approaches. Standard therapy alone may not be sufficient for this group without explicit stigma-focused components.
- Not all therapy is stigma-conscious. A therapist focused entirely on symptom management may not proactively address the internalised beliefs that prevent full engagement. Stigma reduction requires intention from both client and therapist.
- Disclosure remains difficult. Even after beginning therapy, many clients withhold significant information due to ongoing shame. Progress in therapy depends on disclosure, and stigma directly inhibits it.
- Structural inequalities persist. Black, Asian, and minority ethnic communities in the UK continue to report higher levels of stigma and lower levels of trust in mental health services, reflecting inequalities that individual therapy alone cannot resolve.
Pro Tip: When selecting a therapist, ask specifically whether they have experience supporting clients who are managing mental health stigma. A therapist who can name this as part of their approach is likely to create a more stigma-conscious environment from the outset.
For practical strategies beyond the therapy room, mental health management tips for UK adults offer grounded, accessible guidance that complements clinical support. Peer communities and workplace mental health networks can also play a role in building confidence between sessions. Exploring self-help resources for flexible UK support can provide additional structure when professional sessions alone feel insufficient.
What most articles miss about therapy and mental health stigma
Most discussions of this topic treat therapy as a uniform solution. Apply therapy, reduce stigma. The reality is more specific, and missing that specificity leads to misplaced expectations.
Stigma reduction is not a side effect of therapy. It is an outcome that requires the right conditions. A therapist who is skilled at treating depression through structured CBT may not have training in addressing the shame beliefs that surround that depression. These are related but distinct competencies. Choosing a therapist with explicit awareness of stigma dynamics, or seeking out formats that include lived experience and group contact, changes the outcome profile significantly.
There is also a timing dimension that rarely gets discussed. Early in therapy, stigma often increases before it decreases. A person beginning to confront internalised shame may feel worse temporarily. This is not a sign of failure. It is a known feature of the process. Managing that initial discomfort requires preparation and, ideally, a therapist who names it in advance.
Group therapy tends to be underutilised in the UK relative to its evidence base for stigma reduction. The discomfort of sharing in a group context is real, but the mechanism of social contact, which means hearing others' stories and having one's own story received without judgement, is among the most powerful available. This is worth considering when thinking about prioritising mental health as a long-term goal rather than a short-term fix.
The honest position is this: therapy reduces stigma when it is designed to do so, when the individual is ready to engage with that dimension, and when the format matches the person's specific needs. That is not a narrow window. It is wide enough for most people to find their way through. But it requires informed choice, not just access.
Find accessible therapy to break the stigma
Understanding how stigma operates and how therapy addresses it is the first step. Taking action on that knowledge is the next. Many UK adults who would benefit from therapy have not yet started, not because services are unavailable, but because stigma makes the decision feel too exposed or too difficult.
MySafeTherapy connects you with BACP, UKCP, and NCPS-registered therapists through confidential, flexible formats including video, chat, and avatar-based sessions. Sessions are available evenings and weekends, and you can begin therapy online from home, on your terms. No waiting room. No visibility concerns. Just professional, accredited support built around your comfort and confidentiality. Pricing is transparent, therapist switching is straightforward, and AI journaling tools support your progress between sessions.
Frequently asked questions
How does therapy address my fear of judgement?
Therapy creates a confidential space where your experiences are accepted without judgement, and therapists are trained to address internalised stigma and self-critical beliefs directly within sessions.
Can online therapy help reduce stigma as much as in-person support?
Yes, particularly because accessible online and self-referral options remove the visibility barriers associated with entering a physical clinic, making help-seeking feel significantly safer for many people.
Does therapy reduce stigma for everyone?
Outcomes are not uniform. Stigma intervention results are heterogeneous, and depend on the individual's specific concerns, their readiness to engage, and the therapeutic format used.
What should I do if I still feel ashamed to seek help?
Consider group therapy or formats that incorporate shared experience, since social contact and peer stories reduce internalised stigma and can make it easier to accept support without shame.